Exhibit 99.1 Corporate Presentation JANUARY 2024 © 2024 Cabaletta Bio. All rights reserved.
Disclaimer The following presentation, including any printed or electronic copy of these slides, the talks given by the presenters, the information communicated during any delivery of the presentation and any question and answer session and any document or material distributed at or in connection with the presentation (collectively, the “Presentation”) has been prepared by Cabaletta Bio, Inc. (“we,” “us,” “our,” “Cabaletta” or the “Company”) and is made for informational purposes only. This Presentation does not purport to be a prospectus, to be complete or to contain all of the information you may desire. Statements contained herein are made as of the date of this Presentation unless stated otherwise, and this Presentation shall not under any circumstances create an implication that the information contained herein is correct as of any time after such date or that information will be updated or revised to reflect information that subsequently becomes available or changes occurring after the date hereof. This Presentation may contain “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995 relating to our business, operations, and financial conditions, and include, but are not limited to, express or implied statements regarding our current beliefs, expectations and assumptions regarding: our business, future plans and strategies for our CAAR T and CARTA technologies; our ability to grow our autoimmune-focused pipeline; the ability to capitalize on and potential benefits resulting from our research and translational insights; the anticipated market opportunities for CABA-201 in patients with autoimmune diseases; the Company’s business plans and objectives; our expectations around the potential success and therapeutic benefits of CABA-201, including our belief that CABA-201 may enable an “immune system reset”; our plans for Phase 1/2 clinical trials of CABA-201 in patients with systemic lupus erythematosus (SLE), myositis, SSc, and generalized myasthenia gravis (gMG), including our anticipated progress, enrollment, clinical trial design, and ability to leverage our experience in autoimmune cell therapy; our planned initial clinical data read-out in the first half of 2024 for patients with myositis and SLE treated with CABA-201; our planned initial clinical data read-out in the second half of 2024 for patients with SSc and gMG treated with CABA-201; our ability to enroll the requisite number of patients, dose each dosing cohort in the intended manner, and advance the trial as planned in our Phase 1/2 clinical trials of CABA- 201; the ability to retain and recognize the intended incentives conferred by any Fast Track Designations for CABA-201; the timing any planned regulatory filings for our development programs; the progress and results of our DesCAARTes™ Phase 1 trial, including the significance and impact around reported safety and clinical and translational data of cohorts from our DesCAARTes™ and MusCAARTes™ Phase 1; the therapeutic potential and clinical benefits of our product candidates; the expectation that Cabaletta may improve outcomes for patients suffering from SLE, SSc, myositis, gMG, mucosal pemphigus vulgaris, MuSK myasthenia gravis, or other autoimmune diseases; the ability of our clinical strategy to reduce risk, maximize reach and accelerate timelines of our Phase 1/2 clinical trials of CABA-201; our ability to optimize and scale the patient and provider experience; our ability to successfully complete our preclinical and clinical studies for our product candidates, including our ability to enroll the requisite number of patients, dose each dosing cohort in the intended manner, and progress the trial; our ability to obtain and maintain regulatory approval of our product candidates, including our expectations regarding the intended incentives conferred by and ability to retain Orphan Drug Designation and Fast Track Designations for our product candidates, as applicable; our ability to accelerate our pipeline and to develop meaningful therapies for patients, including in collaboration with academic and industry partners and the ability to optimize such collaborations on our development programs; our ability to contract with third-party suppliers and manufacturers, implement an enhanced manufacturing process and further develop our internal manufacturing strategy, capabilities and facilities; our potential commercial opportunities, including value and addressable market, for our product candidates; and our expectations regarding our use of capital and other financial results, including our ability to fund operations into the first half of 2026. Words such as, but not limited to, “look forward to,” “believe,” “expect,” “anticipate,” “estimate,” “intend,” “plan,” “would,” “should” and “could,” and similar expressions or words, identify forward-looking statements. Various risks, uncertainties and assumptions could cause actual results to differ materially from those anticipated or implied in our forward-looking statements. Such risks and uncertainties include, but are not limited to, risks related to the success, cost, and timing of our product candidate development activities and preclinical studies and clinical trials, risks related to our ability to demonstrate sufficient evidence of safety, efficacy and tolerability in our preclinical studies and clinical trials of CABA-201, DSG3-CAART and MuSK-CAART, the risk that the results observed with the similarly-designed construct, including, but not limited to, due to dosing regimen, are not indicative of the results we seek to achieve with CABA-201, our plans to evaluate additional cohorts in the DesCAARTes™ trial, including a cohort implementing a pre-treatment regimen, the risk that signs of biologic activity or persistence may not inform long-term results, the risk that persistence observed with effective CART-19 oncology studies in combination with lymphodepletion is not indicative of, or applicable to, clinical responses in patients with mPV, risks related to clinical trial site activation or enrollment rates that are lower than expected, our ability to protect and maintain our intellectual property position, risks related to our relationships with third parties, uncertainties related to regulatory agencies’ evaluation of regulatory filings and other information related to our product candidates, our ability to retain and recognize the intended incentives conferred by any Orphan Drug Designations and Fast Track Designations, risks related to regulatory filings and potential clearance, the risk that any one or more of our product candidates will not be successfully developed and commercialized, the risk that the results of preclinical studies or clinical studies will not be predictive of future results in connection with future studies, and risks related to volatile market and economic conditions and public health crises. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. Except as required by applicable law, we do not plan to publicly update or revise any forward-looking statements contained herein, whether as a result of any new information, future events, changed circumstances or otherwise. Although we believe the expectations reflected in such forward-looking statements are reasonable, we can give no assurance that such expectations will prove to be correct. Accordingly, you are cautioned not to place undue reliance on these forward-looking statements. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-looking statements. For a discussion of these and other risks and uncertainties, and other important factors, any of which could cause our actual results to differ materially from those contained in the forward-looking statements, see the section entitled Risk Factors in our most recent annual report on Form 10-K, as well as discussions of potential risks, uncertainties, and other important factors in our other and subsequent filings with the Securities and Exchange Commission. Certain information contained in this Presentation relates to or is based on studies, publications, surveys and other data obtained from third-party sources and the Company’s own internal estimates and research. While the Company believes these third-party sources to be reliable as of the date of this Presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third-party sources. The Company is the owner of various trademarks, trade names and service marks. Certain other trademarks, trade names and service marks appearing in this Presentation are the property of third parties. Solely for convenience, the trademarks and trade names in this Presentation are referred to without the ® and TM symbols, but such references should not be construed as any indicator that their respective owners will not assert, to the fullest extent under applicable law, their rights thereto. 2
Develop and launch the first curative targeted cellular therapies for patients with autoimmune diseases 3 3
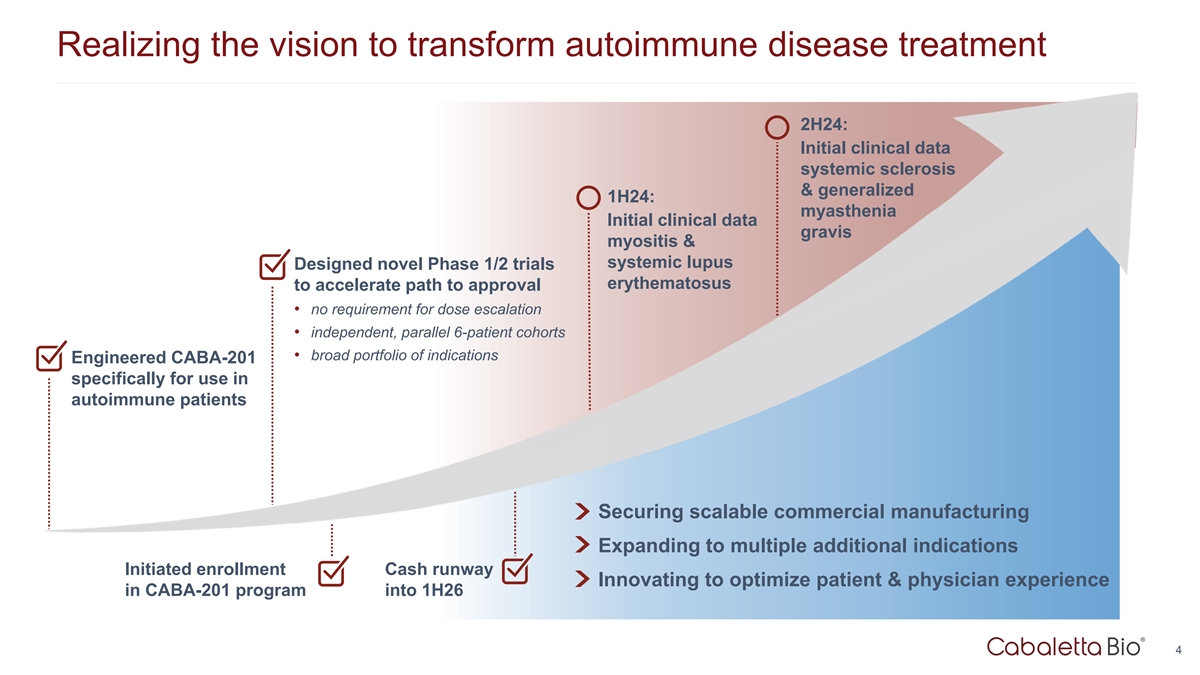
Realizing the vision to transform autoimmune disease treatment 2H24: Initial clinical data systemic sclerosis & generalized 1H24: myasthenia Initial clinical data gravis myositis & systemic lupus Designed novel Phase 1/2 trials erythematosus to accelerate path to approval • no requirement for dose escalation • independent, parallel 6-patient cohorts • broad portfolio of indications Engineered CABA-201 specifically for use in autoimmune patients Securing scalable commercial manufacturing Expanding to multiple additional indications Initiated enrollment Cash runway Innovating to optimize patient & physician experience in CABA-201 program into 1H26 4
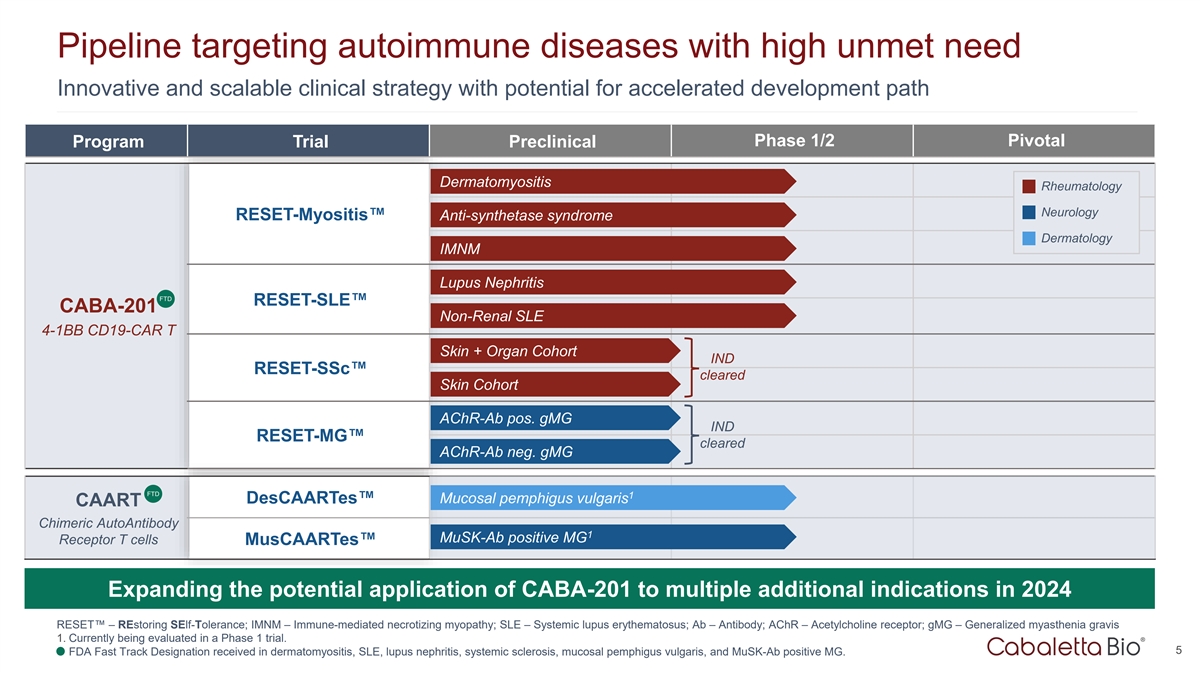
Pipeline targeting autoimmune diseases with high unmet need Innovative and scalable clinical strategy with potential for accelerated development path Phase 1/2 Pivotal Program Trial Preclinical Dermatomyositis Rheumatology Neurology RESET-Myositis™ Anti-synthetase syndrome Dermatology IMNM Lupus Nephritis FTD RESET-SLE™ CABA-201 Non-Renal SLE 4-1BB CD19-CAR T Skin + Organ Cohort IND RESET-SSc™ cleared Skin Cohort AChR-Ab pos. gMG IND RESET-MG™ cleared AChR-Ab neg. gMG FTD 1 DesCAARTes™ Mucosal pemphigus vulgaris CAART Chimeric AutoAntibody 1 MuSK-Ab positive MG Receptor T cells MusCAARTes™ Expanding the potential application of CABA-201 to multiple additional indications in 2024 RESET™ – REstoring SElf-Tolerance; IMNM – Immune-mediated necrotizing myopathy; SLE – Systemic lupus erythematosus; Ab – Antibody; AChR – Acetylcholine receptor; gMG – Generalized myasthenia gravis 1. Currently being evaluated in a Phase 1 trial. 5 2. FDA Fast Track Designation received in dermatomyositis, SLE, lupus nephritis, systemic sclerosis, mucosal pemphigus vulgaris, and MuSK-Ab positive MG.
Chimeric Antigen Receptor T Cells for Autoimmunity CABA-201 6
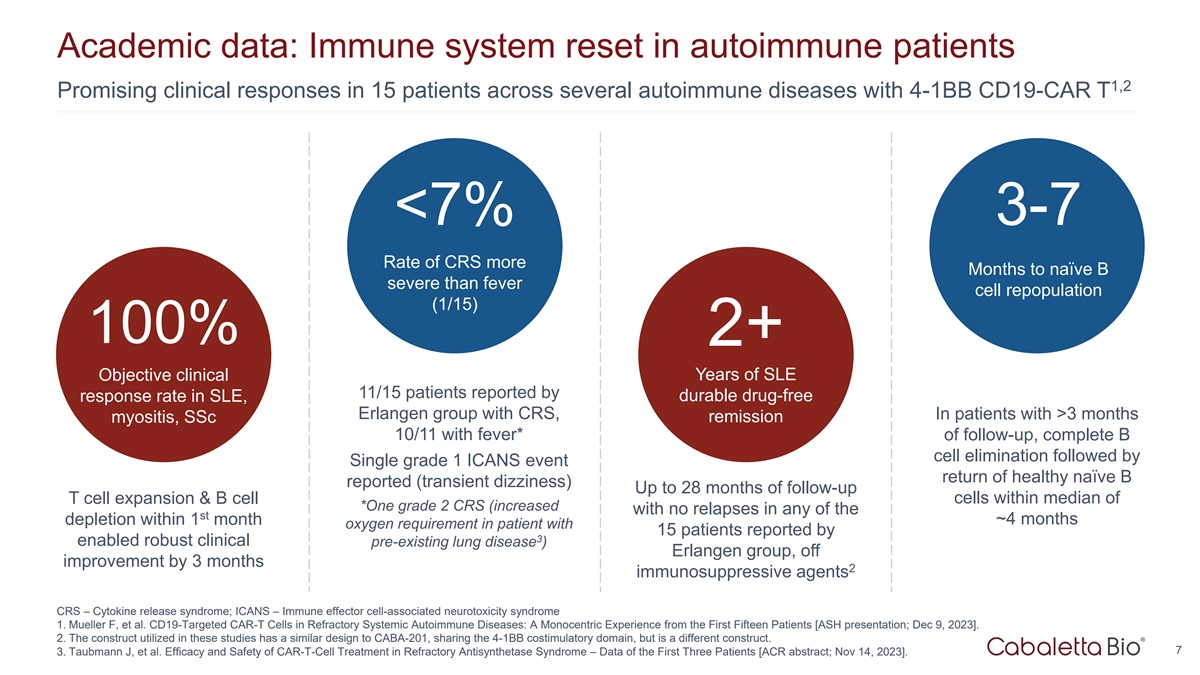
Academic data: Immune system reset in autoimmune patients 1,2 Promising clinical responses in 15 patients across several autoimmune diseases with 4-1BB CD19-CAR T <7% 3-7 Rate of CRS more Months to naïve B severe than fever cell repopulation (1/15) 100% 2+ Years of SLE Objective clinical 11/15 patients reported by durable drug-free response rate in SLE, Erlangen group with CRS, In patients with >3 months myositis, SSc remission 10/11 with fever* of follow-up, complete B cell elimination followed by Single grade 1 ICANS event return of healthy naïve B reported (transient dizziness) Up to 28 months of follow-up T cell expansion & B cell cells within median of *One grade 2 CRS (increased with no relapses in any of the st depletion within 1 month ~4 months oxygen requirement in patient with 15 patients reported by 3 enabled robust clinical pre-existing lung disease ) Erlangen group, off improvement by 3 months 2 immunosuppressive agents CRS – Cytokine release syndrome; ICANS – Immune effector cell-associated neurotoxicity syndrome 1. Mueller F, et al. CD19-Targeted CAR-T Cells in Refractory Systemic Autoimmune Diseases: A Monocentric Experience from the First Fifteen Patients [ASH presentation; Dec 9, 2023]. 2. The construct utilized in these studies has a similar design to CABA-201, sharing the 4-1BB costimulatory domain, but is a different construct. 7 3. Taubmann J, et al. Efficacy and Safety of CAR-T-Cell Treatment in Refractory Antisynthetase Syndrome – Data of the First Three Patients [ACR abstract; Nov 14, 2023].
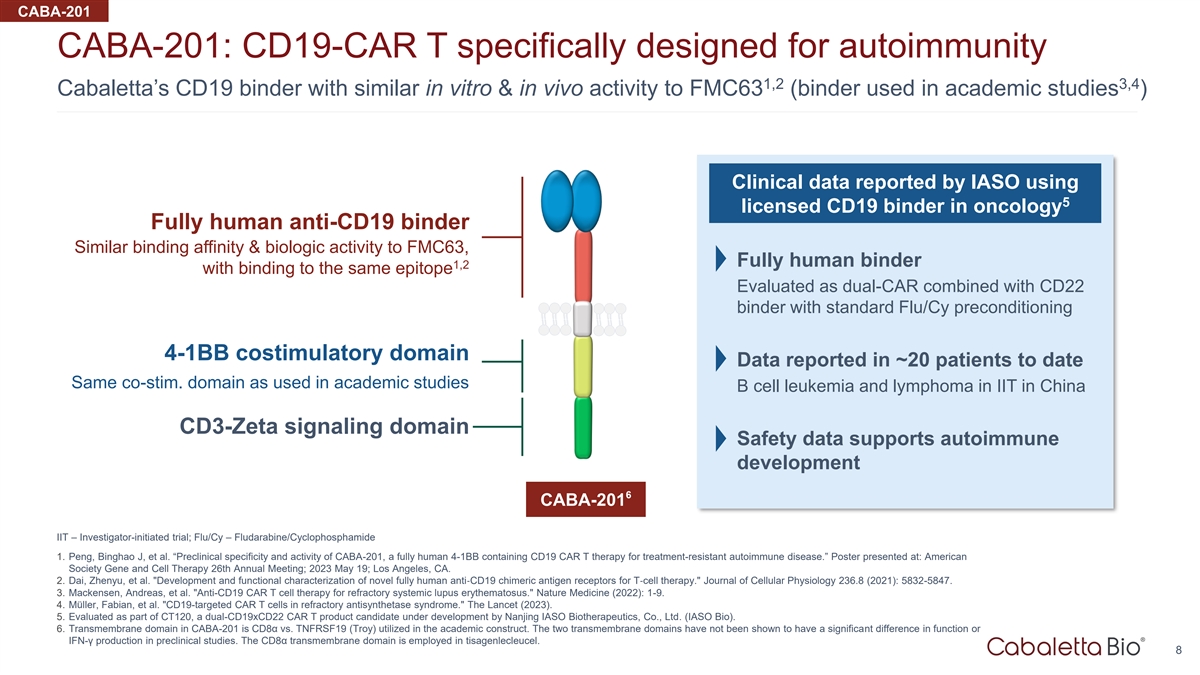
CABA-201 CABA-201: CD19-CAR T specifically designed for autoimmunity 1,2 3,4 Cabaletta’s CD19 binder with similar in vitro & in vivo activity to FMC63 (binder used in academic studies ) Clinical data reported by IASO using 5 licensed CD19 binder in oncology Fully human anti-CD19 binder Similar binding affinity & biologic activity to FMC63, Fully human binder 1,2 with binding to the same epitope Evaluated as dual-CAR combined with CD22 binder with standard Flu/Cy preconditioning 4-1BB costimulatory domain Data reported in ~20 patients to date Same co-stim. domain as used in academic studies B cell leukemia and lymphoma in IIT in China CD3-Zeta signaling domain Safety data supports autoimmune development 6 CABA-201 IIT – Investigator-initiated trial; Flu/Cy – Fludarabine/Cyclophosphamide 1. Peng, Binghao J, et al. “Preclinical specificity and activity of CABA-201, a fully human 4-1BB containing CD19 CAR T therapy for treatment-resistant autoimmune disease.” Poster presented at: American Society Gene and Cell Therapy 26th Annual Meeting; 2023 May 19; Los Angeles, CA. 2. Dai, Zhenyu, et al. Development and functional characterization of novel fully human anti‐CD19 chimeric antigen receptors for T‐cell therapy. Journal of Cellular Physiology 236.8 (2021): 5832-5847. 3. Mackensen, Andreas, et al. Anti-CD19 CAR T cell therapy for refractory systemic lupus erythematosus. Nature Medicine (2022): 1-9. 4. Müller, Fabian, et al. CD19-targeted CAR T cells in refractory antisynthetase syndrome. The Lancet (2023). 5. Evaluated as part of CT120, a dual-CD19xCD22 CAR T product candidate under development by Nanjing IASO Biotherapeutics, Co., Ltd. (IASO Bio). 6. Transmembrane domain in CABA-201 is CD8α vs. TNFRSF19 (Troy) utilized in the academic construct. The two transmembrane domains have not been shown to have a significant difference in function or IFN-γ production in preclinical studies. The CD8α transmembrane domain is employed in tisagenlecleucel. 8
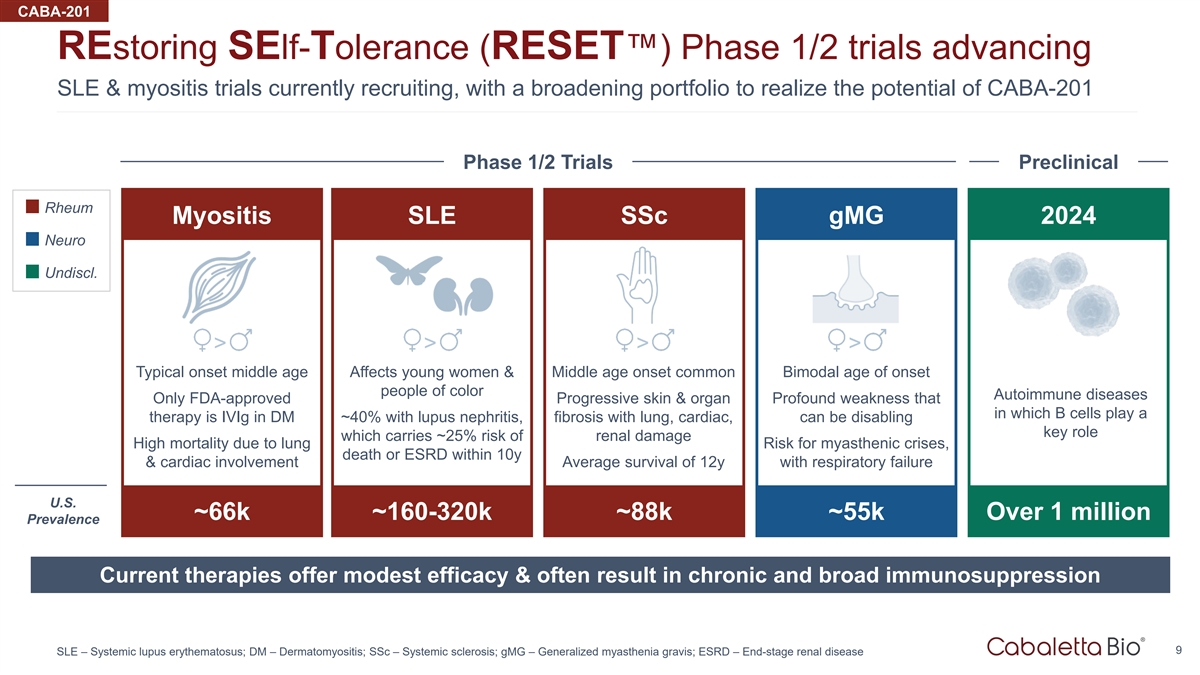
CABA-201 REstoring SElf-Tolerance (RESET™) Phase 1/2 trials advancing SLE & myositis trials currently recruiting, with a broadening portfolio to realize the potential of CABA-201 Phase 1/2 Trials Preclinical Rheum Myositis SLE SSc gMG 2024 Neuro Undiscl. > > > > Typical onset middle age Affects young women & Middle age onset common Bimodal age of onset people of color Autoimmune diseases Only FDA-approved Progressive skin & organ Profound weakness that in which B cells play a therapy is IVIg in DM ~40% with lupus nephritis, fibrosis with lung, cardiac, can be disabling key role which carries ~25% risk of renal damage High mortality due to lung Risk for myasthenic crises, death or ESRD within 10y & cardiac involvement Average survival of 12y with respiratory failure U.S. ~66k ~160-320k ~88k ~55k Over 1 million Prevalence Current therapies offer modest efficacy & often result in chronic and broad immunosuppression 9 SLE – Systemic lupus erythematosus; DM – Dermatomyositis; SSc – Systemic sclerosis; gMG – Generalized myasthenia gravis; ESRD – End-stage renal disease
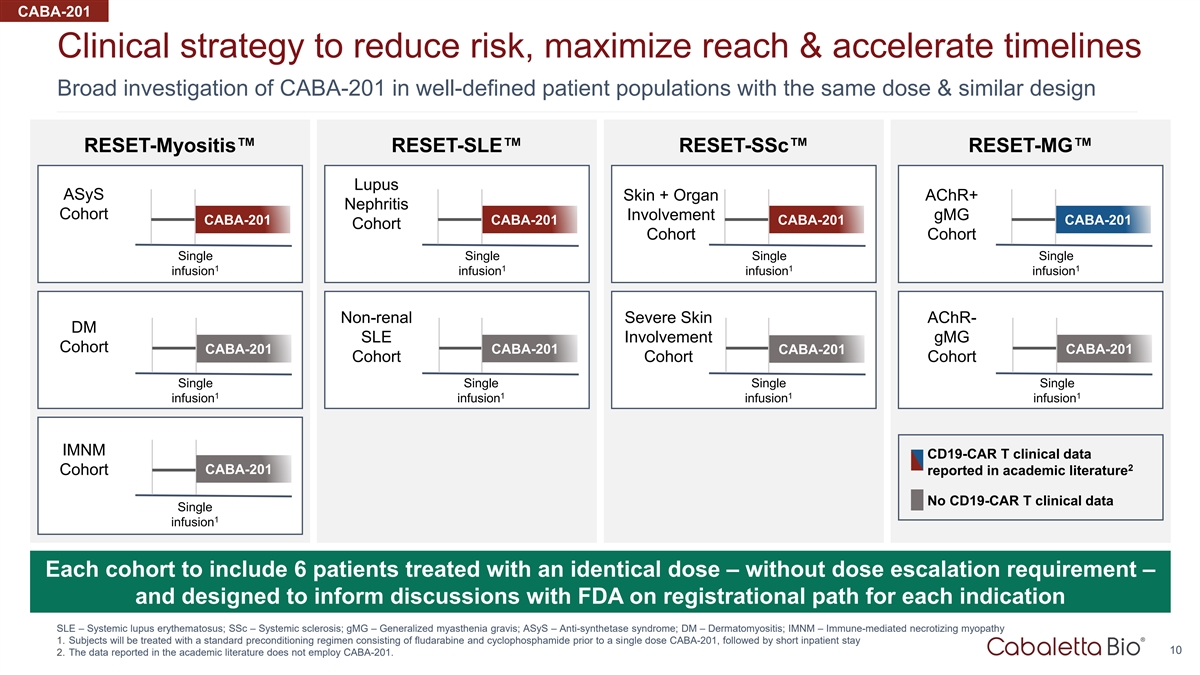
CABA-201 Clinical strategy to reduce risk, maximize reach & accelerate timelines Broad investigation of CABA-201 in well-defined patient populations with the same dose & similar design RESET-Myositis™ RESET-SLE™ RESET-SSc™ RESET-MG™ Lupus ASyS Skin + Organ AChR+ Nephritis Cohort Involvement gMG CABA-201 CABA-201 CABA-201 CABA-201 Cohort Cohort Cohort Single Single Single Single 1 1 1 1 infusion infusion infusion infusion Non-renal Severe Skin AChR- DM SLE Involvement gMG Cohort CABA-201 CABA-201 CABA-201 CABA-201 Cohort Cohort Cohort Single Single Single Single 1 1 1 1 infusion infusion infusion infusion IMNM CD19-CAR T clinical data 2 CABA-201 Cohort reported in academic literature No CD19-CAR T clinical data Single 1 infusion Each cohort to include 6 patients treated with an identical dose – without dose escalation requirement – and designed to inform discussions with FDA on registrational path for each indication SLE – Systemic lupus erythematosus; SSc – Systemic sclerosis; gMG – Generalized myasthenia gravis; ASyS – Anti-synthetase syndrome; DM – Dermatomyositis; IMNM – Immune-mediated necrotizing myopathy 1. Subjects will be treated with a standard preconditioning regimen consisting of fludarabine and cyclophosphamide prior to a single dose CABA-201, followed by short inpatient stay 10 2. The data reported in the academic literature does not employ CABA-201.
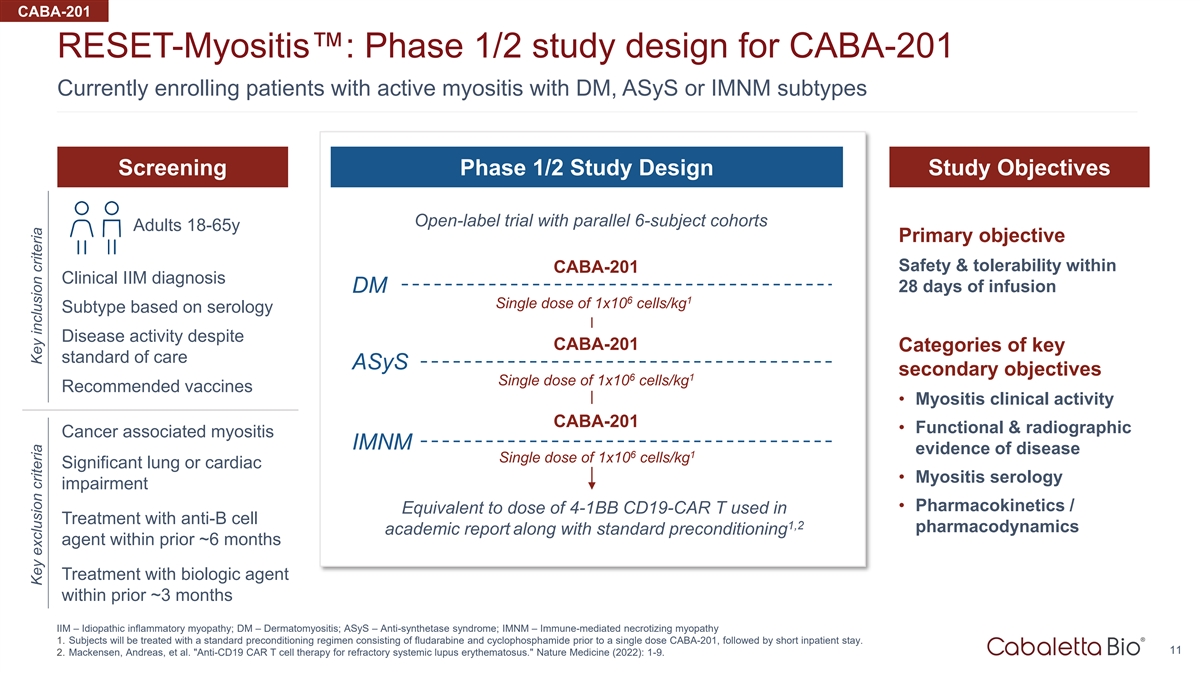
CABA-201 RESET-Myositis™: Phase 1/2 study design for CABA-201 Currently enrolling patients with active myositis with DM, ASyS or IMNM subtypes Screening Phase 1/2 Study Design Study Objectives Open-label trial with parallel 6-subject cohorts Adults 18-65y Primary objective Safety & tolerability within CABA-201 Clinical IIM diagnosis DM 28 days of infusion 6 1 Single dose of 1x10 cells/kg Subtype based on serology Disease activity despite CABA-201 Categories of key standard of care ASyS secondary objectives 6 1 Single dose of 1x10 cells/kg Recommended vaccines • Myositis clinical activity CABA-201 • Functional & radiographic Cancer associated myositis IMNM evidence of disease 6 1 Single dose of 1x10 cells/kg Significant lung or cardiac • Myositis serology impairment • Pharmacokinetics / Equivalent to dose of 4-1BB CD19-CAR T used in Treatment with anti-B cell 1,2 pharmacodynamics academic report along with standard preconditioning agent within prior ~6 months Treatment with biologic agent within prior ~3 months IIM – Idiopathic inflammatory myopathy; DM – Dermatomyositis; ASyS – Anti-synthetase syndrome; IMNM – Immune-mediated necrotizing myopathy 1. Subjects will be treated with a standard preconditioning regimen consisting of fludarabine and cyclophosphamide prior to a single dose CABA-201, followed by short inpatient stay. 11 2. Mackensen, Andreas, et al. Anti-CD19 CAR T cell therapy for refractory systemic lupus erythematosus. Nature Medicine (2022): 1-9. Key exclusion criteria Key inclusion criteria
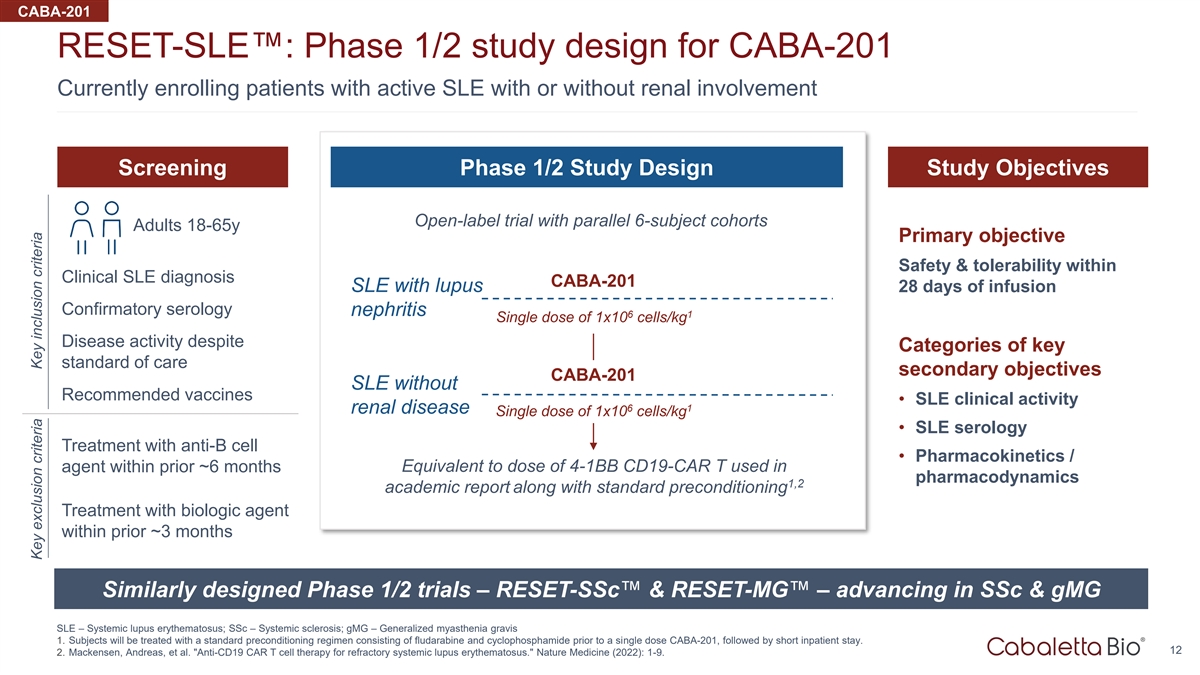
CABA-201 RESET-SLE™: Phase 1/2 study design for CABA-201 Currently enrolling patients with active SLE with or without renal involvement Screening Phase 1/2 Study Design Study Objectives Open-label trial with parallel 6-subject cohorts Adults 18-65y Primary objective Safety & tolerability within Clinical SLE diagnosis CABA-201 SLE with lupus 28 days of infusion Confirmatory serology nephritis 6 1 Single dose of 1x10 cells/kg Disease activity despite Categories of key standard of care secondary objectives CABA-201 SLE without Recommended vaccines • SLE clinical activity 6 1 renal disease Single dose of 1x10 cells/kg • SLE serology Treatment with anti-B cell • Pharmacokinetics / agent within prior ~6 months Equivalent to dose of 4-1BB CD19-CAR T used in pharmacodynamics 1,2 academic report along with standard preconditioning Treatment with biologic agent within prior ~3 months Similarly designed Phase 1/2 trials – RESET-SSc™ & RESET-MG™ – advancing in SSc & gMG SLE – Systemic lupus erythematosus; SSc – Systemic sclerosis; gMG – Generalized myasthenia gravis 1. Subjects will be treated with a standard preconditioning regimen consisting of fludarabine and cyclophosphamide prior to a single dose CABA-201, followed by short inpatient stay. 12 2. Mackensen, Andreas, et al. Anti-CD19 CAR T cell therapy for refractory systemic lupus erythematosus. Nature Medicine (2022): 1-9. Key exclusion criteria Key inclusion criteria
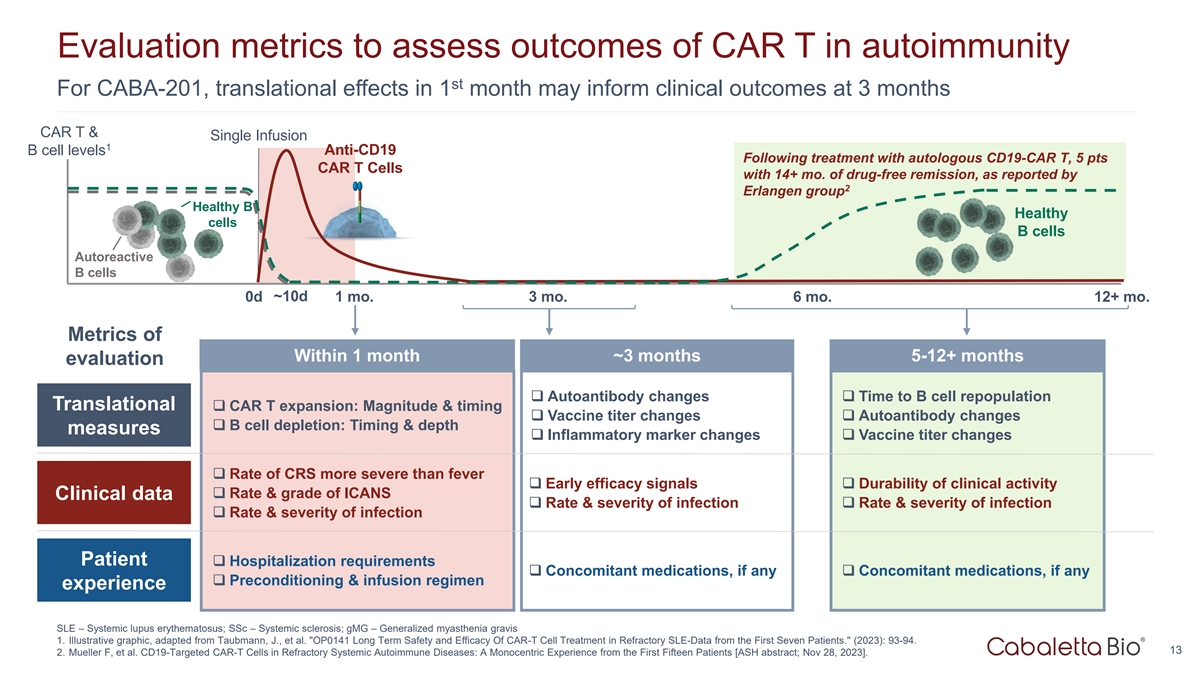
Evaluation metrics to assess outcomes of CAR T in autoimmunity st For CABA-201, translational effects in 1 month may inform clinical outcomes at 3 months CAR T & Single Infusion 1 B cell levels Anti-CD19 Following treatment with autologous CD19-CAR T, 5 pts CAR T Cells with 14+ mo. of drug-free remission, as reported by 2 Erlangen group Healthy B Healthy cells B cells Autoreactive B cells ~10d 0d 1 mo. 3 mo. 6 mo. 12+ mo. Metrics of Within 1 month ~3 months 5-12+ months evaluation ❑ Autoantibody changes❑ Time to B cell repopulation Translational ❑ CAR T expansion: Magnitude & timing ❑ Vaccine titer changes❑ Autoantibody changes ❑ B cell depletion: Timing & depth measures ❑ Inflammatory marker changes❑ Vaccine titer changes ❑ Rate of CRS more severe than fever ❑ Early efficacy signals❑ Durability of clinical activity ❑ Rate & grade of ICANS Clinical data ❑ Rate & severity of infection❑ Rate & severity of infection ❑ Rate & severity of infection Patient ❑ Hospitalization requirements ❑ Concomitant medications, if any❑ Concomitant medications, if any ❑ Preconditioning & infusion regimen experience SLE – Systemic lupus erythematosus; SSc – Systemic sclerosis; gMG – Generalized myasthenia gravis 1. Illustrative graphic, adapted from Taubmann, J., et al. OP0141 Long Term Safety and Efficacy Of CAR-T Cell Treatment in Refractory SLE-Data from the First Seven Patients. (2023): 93-94. 13 2. Mueller F, et al. CD19-Targeted CAR-T Cells in Refractory Systemic Autoimmune Diseases: A Monocentric Experience from the First Fifteen Patients [ASH abstract; Nov 28, 2023].
Manufacturing strategy Staged approach allows for efficient allocation of capital while leveraging experienced partners Early Phase: Late Phase & Commercial: Penn, CDMOs & CABA Process Scale-Up & Commercialization Data-gated, staged investment Ongoing • Penn has reliably provided timely product for years • Evaluating potential paths to commercial-ready manufacturing: • Commercial CDMO partnerships have expanded • Expansion of CDMO relationships our vector and cell product supply • Cabaletta-operated facility • Strategic partnership(s) • Continuous focus on innovations to address scale Preparations ongoing to implement commercial-ready process in advance of pivotal studies 14
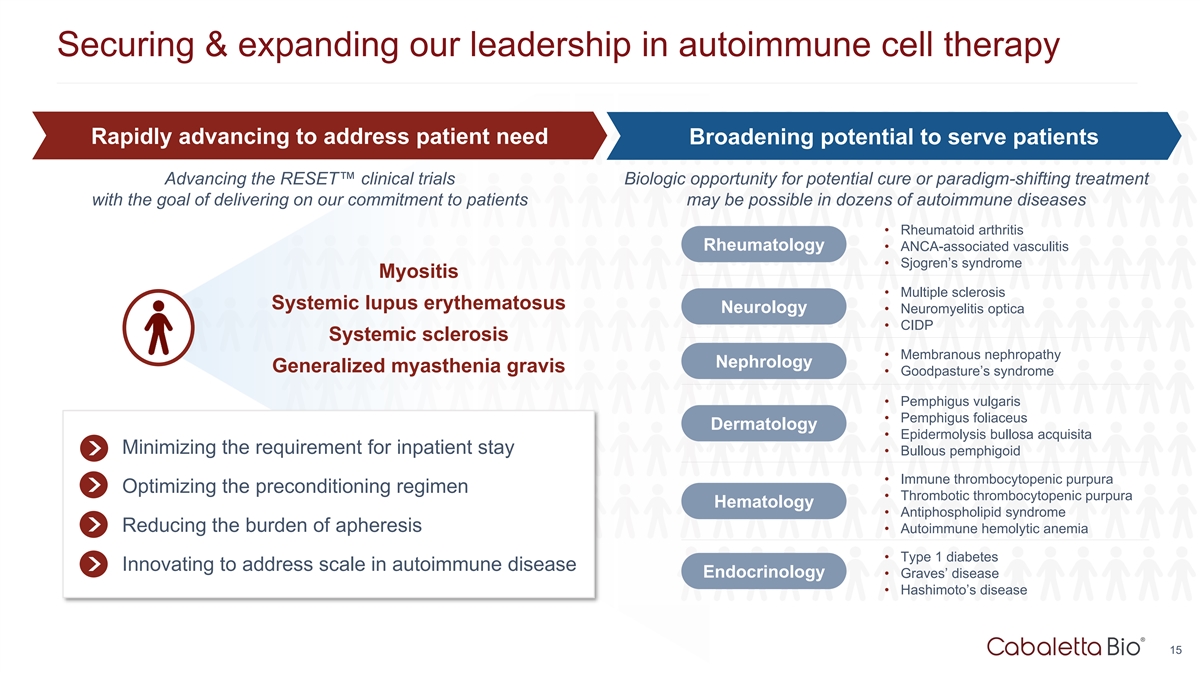
Securing & expanding our leadership in autoimmune cell therapy Rapidly advancing to address patient need Broadening potential to serve patients Advancing the RESET™ clinical trials Biologic opportunity for potential cure or paradigm-shifting treatment with the goal of delivering on our commitment to patients may be possible in dozens of autoimmune diseases • Rheumatoid arthritis Rheumatology • ANCA-associated vasculitis • Sjogren’s syndrome Myositis • Multiple sclerosis Systemic lupus erythematosus Neurology • Neuromyelitis optica • CIDP Systemic sclerosis • Membranous nephropathy Nephrology Generalized myasthenia gravis • Goodpasture’s syndrome • Pemphigus vulgaris • Pemphigus foliaceus Dermatology • Epidermolysis bullosa acquisita Minimizing the requirement for inpatient stay • Bullous pemphigoid • Immune thrombocytopenic purpura Optimizing the preconditioning regimen • Thrombotic thrombocytopenic purpura Hematology • Antiphospholipid syndrome Reducing the burden of apheresis • Autoimmune hemolytic anemia • Type 1 diabetes Innovating to address scale in autoimmune disease Endocrinology • Graves’ disease • Hashimoto’s disease 15
Corporate Summary 16

Cabaletta Bio leadership LEADERSHIP TEAM Steven Nichtberger, M.D. Samik Basu, M.D. Gwendolyn Binder, Ph.D. David J. Chang, M.D., M.P.H., FACR Arun Das, M.D. President, CEO & Chairman Chief Scientific Officer President, Science & Technology Chief Medical Officer Chief Business Officer Michael Gerard Heather Harte-Hall Anup Marda Martha O’Connor General Counsel Chief Compliance Officer Chief Financial Officer Chief HR Officer BOARD OF DIRECTORS SCIENTIFIC ADVISORY BOARD Steven Nichtberger, M.D. Richard Henriques Aimee Payne, M.D., Ph.D. Michael C. Milone, M.D., Ph.D. Co-Founder and Co-Chair Co-Founder and Co-Chair Catherine Bollard, M.D. Mark Simon Brian Daniels, M.D. Georg Schett, M.D. Scott Brun, M.D. Shawn Tomasello Carl June, M.D. Jay Siegel, M.D. Iain McInnes, Ph.D., FRCP, FRSE, FMedSci Drew Weissman, M.D., Ph.D. Track record of operational success evaluating novel cell therapy candidates in autoimmunity across preclinical, clinical, manufacturing & regulatory domains 17
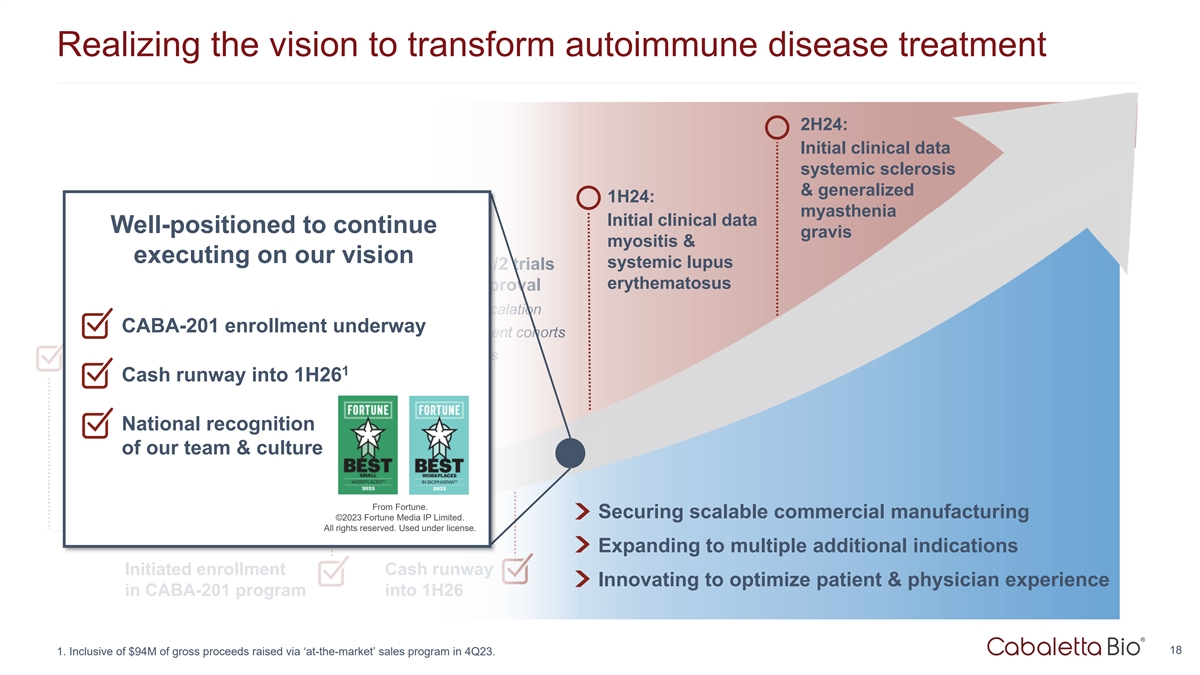
Realizing the vision to transform autoimmune disease treatment 2H24: Initial clinical data systemic sclerosis & generalized 1H24: myasthenia Initial clinical data Well-positioned to continue gravis myositis & executing on our vision systemic lupus Designed novel Phase 1/2 trials erythematosus to accelerate path to approval • no requirement for dose escalation CABA-201 enrollment underway • independent, parallel 6-patient cohorts • broad portfolio of indications Eng En inee gineer red ed CABA -201 1 Cash runway into 1H26 spec CABA ifical -201 ly for use in autoimmu specifical ne ly patien for ts use in National recognition autoimmune of our team & culture patients From Fortune. Securing scalable commercial manufacturing ©2023 Fortune Media IP Limited. All rights reserved. Used under license. Expanding to multiple additional indications Initiated enrollment Cash runway Innovating to optimize patient & physician experience in CABA-201 program into 1H26 18 1. Inclusive of $94M of gross proceeds raised via ‘at-the-market’ sales program in 4Q23.
Corporate Presentation JANUARY 2024 © 2024 Cabaletta Bio. All rights reserved.